Figure legend from original manuscript:
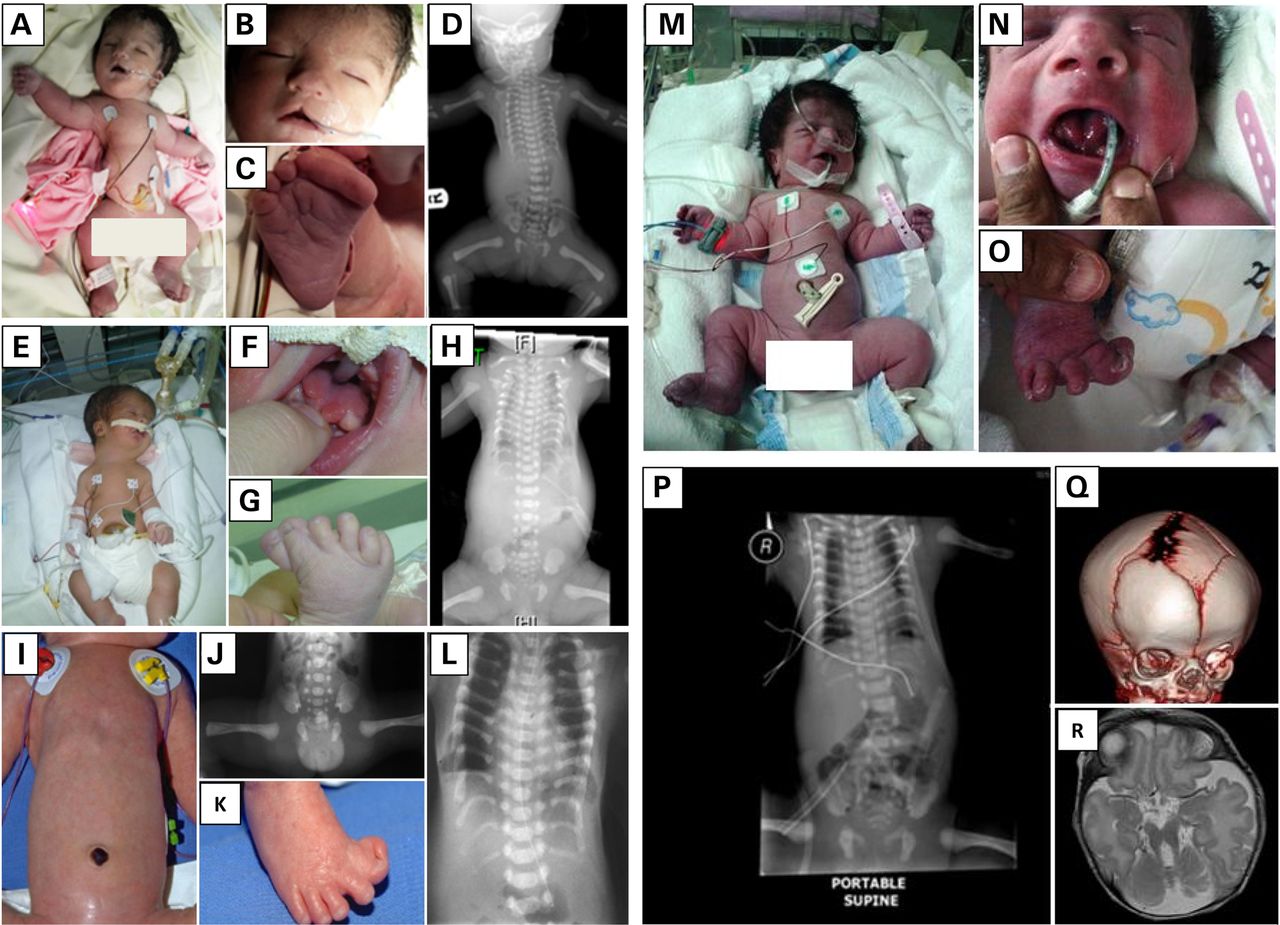
Fig. 1. Clinical images of the study families. (A–D) Postnatal clinical photograph and radiological imaging of the index
case from Family 1 showing severely narrow chest and thorax, mild cleft lip (notch), short limbs and synpolydactyly.
(E–H) Postnatal clinical photograph and radiological imaging of the index case from Family 2 showing very narrow chest,
short extremities, synpolydactyly, tongue hamartoma (lobulated tongue) and omphalocele. (I–L) Postnatal clinical photograph
and radiological imaging of the individual Family 3_II:1 showing long and narrow thorax with short horizontal ribs,
dysplastic pelvis with acetabular spurs and hexadactyly of the feet. (M–R) Postnatal clinical photograph, radiological
imaging, 3D skull computed tomography and MRI of the index case from Family 4 showing coarse facies, midface hypoplasia,
partially bifid tongue, polydactyly, short tubular bones, bell-shaped thorax with short ribs, unilateral coronal craniosynostosis
with prominent and widened anterior and posterior fontanels, and brain vermian hypoplasia with molar-tooth appearance.
Source: Shaheen R et al. (2014) A founder CEP120 mutation in Jeune asphyxiating thoracic dystrophy expands the role of
centriolar proteins in skeletal ciliopathies.
Hum Mol Genet 24(5):1410-1419.
Full text on PubMed.
Back to Jeune syndrome page